 RSS Feed
RSS Feed Twitter
Twitter 10:39 AM
10:39 AM
 Zia
Zia

Neck pain includes general pain and stiffness in the neck region, which can include the neck, shoulders, arms, hands, or head. The muscles can be sore and tense. Patients often report of mild to severe headaches. Most pain is due to the aging of the spine. As the spine ages, the discs can degenerate and herniate. The joints may become arthritic, stenosis can occur (narrowing of the spinal canal), and instability may develop.
There are three types or classifications of neck pain:
1. Axial neck pain
2. Radiculopathy
3. Myelopathy
All three of the types of neck pain can be Acute or Chronic.Acute pain occurs suddenly from an injury or stress. Most of the time neck pain will resolve itself within 7-10 days with rest, ice, and over the counter pain relievers. For symptoms that persist longer than a few weeks, a thorough evaluation by a primary care physician is recommended. The physician will generally obtain x-rays and MRIs, and prescribe conservative therapy. Conservative therapy can include anti-inflammatories, pain medication, injections, physical therapy, acupuncture, and chiropractic care.
Chronic pain is defined as neck pain lasting longer than three months. People who have not found relief through conservative treatments, and suffer from chronic pain may benefit from pain management or surgical intervention.
Now we will briefly describe all the types of neck pain :
1. Axial neck pain

Mechanical or axial neck pain is neck pain that does not radiate into the arms or upper extremities. The pain is located in the neck, base of the skull or occipital area and the back of the shoulders.
Many time, mechanical neck pain is associated with headaches that may radiate into the base of the skull, side of the head (temporal) or around the eyes (periorbital). These headaches are called cervicogenic or neck related headaches.
Mechanical neck pain may have different symptoms; it may be one side or both sides of the neck, cause headaches, stiffness and may lead to restricted motion in on or all directions in the range of neck motion.
Most of the cases of mechanical neck pain involve some type of damage to the muscles or other of the “soft tissues” like ligaments and relief is usually within 4-6 weeks with conservative treatment. Unfortunately, there are about 1/3 of mechanical neck pain cases which do not see relief within this period of time and go on to be considered chronic neck pain. It is these cases where many will seek various methods of treatment and have difficulty in coping with neck pain. Of the approximately 1/3 of cases which progress to the chronic stage of neck pain, about 50% of these will have headaches which radiate to the base of the skull.
There has been much effort to understand the cause(s) of mechanical neck pain, focusing on a better understanding of anatomy and neurology. Unfortunately, most of what is understood about mechanical neck pain is not complete or theoretical and that relates to lack of a very effective treatment that is predictable.
2. Radiculopathy

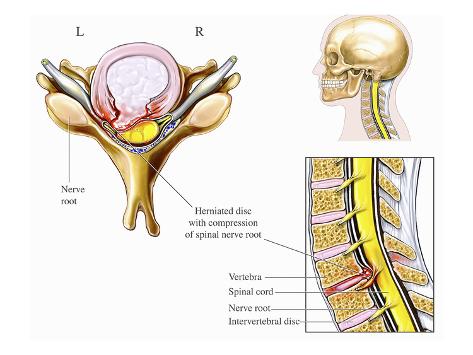
Cervical radiculopathy is the damage or disturbance of nerve function that results if one of the nerve roots near the cervical vertebrae is compressed. Damage to nerve roots in the cervical area can cause pain and the loss of sensation along the nerve's pathway into the arm and hand, depending on where the damaged roots are located.
Causes of Cervical Radiculopathy
Damage can occur as a result of pressure from material from a ruptured disc, degenerative changes in bones, arthritis or other injuries that put pressure on the nerve roots. In middle-aged people, normal degenerative changes in the discs can cause pressure on nerve roots. In younger people, cervical radiculopathy tends to be the result of a ruptured disc, perhaps as a result of trauma. This disc material then compresses or inflames the nerve root, causing pain.
Symptoms of Cervical Radiculopathy
The main symptom of cervical radiculopathy is pain that spreads into the arm, neck, chest, upper back and/or shoulders. A person with radiculopathy may experience muscle weakness and/or numbness or tingling in fingers or hands. Other symptoms may include lack of coordination, especially in the hands.
Treatments of Cervical Radiculopathy
Cervical radiculopathy may be treated with a combination of pain medications such as corticosteroids (powerful anti-inflammatory drugs) or non-steroidal pain medication like ibuprofen or naproxen and physical therapy. Steroids may be prescribed either orally or injected epidurally (into the space above the dura, which is the membrane that surrounds the spinal cord).
Physical therapy might include gentle cervical traction and mobilization, exercises, and other modalities to reduce pain. If significant compression on the nerve exists to the extent that motor weakness results, surgery may be necessary to relieve the pressure.
3. Myelopathy
Myelopathy, also called spinal cord compression, is one of the most common causes of cervical or neck pain in people over age 55 in the United States and possibly the world. Up to 10% of people who have symptoms of spinal stenosis develop myelopathy. The disorder actually comprises several different medical conditions that cause neck pain, including:
- Transverse syndrome
- Motor system syndrome
- Mixed radicular and long tract syndrome
- Partial Brown-Sequard syndrome
- Central cord syndrome
The pain associated with myelopathy may be due to problems in the vertebrae and facet joints of your spine, as well as in the muscles, ligaments, and nerves of your spine.
Causes of Myelopathy
Normal wear and tear is a common cause of myelopathy. In fact, myelopathy is one of the most common causes of neck pain due to aging. As your body gets older, the normal wear and tear of every-day stress on your spine causes degenerative changes to occur. These changes affect your facet joints, intervertebral discs, and ligaments.
As the discs in your spine grow older they begin to dry out and calcify, which causes them to compress and for the space between your facet joints to close up. This puts added stress on the cartilage that keeps the joints in your spine working properly, and causes the cycle of degeneration to continue. Disc degeneration can also lead to a herniated disc, which can put additional pressure on your spine by pressing against your spinal cord or nerve roots. Degeneration and stress can also cause bone spurs to form. This makes your spinal canal narrow, compressing or squeezing your spinal cord.
Another common cause of myelopathy is injury, such as from car accidents, sports, and falls. These injuries often affect the muscles and ligaments that stabilize your spine, and can also cause bone fractures and joint dislocations. Injuries are a common cause of central cord syndrome.
Myelopathy can also be caused by an inflammatory disease like rheumatoid arthritis, which attacks the joints in your spine and typically affects the area of your upper neck. Less common causes of myelopathy include tumors, infections, and congenital abnormalities of the vertebrae which are present at birth.
Symptoms
The most common symptoms of myelopathy include neck stiffness, deep aching pain in one or both sides of your neck and possibly your arms and shoulders, and possibly stiffness and weakness in your legs and difficulty when walking. You may also feel a grating or crackling sensation when you move your neck. Patients with myelopathy commonly experience stabbing pain in their arm, elbow, wrist, or fingers, a dull ache in the arm, or numbness. Myelopathy can also cause position sense loss, which makes you unable to know where your arms are without looking at them, and incontinence. The symptoms of myelopathy progress slowly over many years and may not become evident until your spinal cord has been compressed by at least 30%.
Diagnosis
The first step in diagnosing myelopathy is a medical history and physic al exam . Your doctor will look specifically for problems with your reflexes, particularly to see whether you have an exaggerated or overactive reflex, which is called hyper-reflexia. Your doctor will also check for muscle weakness particularly in your arms, numbness in your arms and hands, and atrophy, which is a condition in which your muscles deteriorate and shrink in size.
If the results of your history and physic al exam lead your doctor to believe you may have myelopathy, additional diagnostic tests may be ordered including X-rays to check the alignment of the vertebrae in your neck, an MRI to look for spinal cord compression, and a myelogram to check for bone spurs and narrowing of your spinal canal. An electromyogram (EMG) may be helpful in excluding other disorders that may cause symptoms similar to myelopathy.
Treatment
Conservative Treatment
Although surgery to decompress the spinal cord is the best treatment for most patients with myelopathy, watchful waiting is an appropriate approach for patients with mild symptoms. If your myelopathy is mild, your doctor may recommend a brace to immobilize your neck (cervical spine), exercises to improve neck strength and flexibility, manipulation, and pain medication such as a nonsteroidal antiinflammatory drug (NSAID). Some experts recommend against conservative treatment for myelopathy because some conservative treatments have been shown to not be helpful, and in some cases to cause neurological complications.
Epidural steroid injection (ESI)
An epidural spinal injection (ESI) can be used to relieve the pain of a muscle strain or sprain, as well as to decrease inflammation. Injections can also help reduce swelling. Steroid injections are a combination of cortisone (a powerful anti-inflammatory steroid) and a local anesthetic that are given through your back into the epidural space. ESI is not always successful in relieving symptoms of inflammation. They are used only when conservative treatments have failed.
Surgical Treatment
The main goal of surgery for myelopathy is to decompress the spine. Your doctor may choose to perform a laminotomy using a posterior approach (through an incision in your back), which opens up the vertebrae in your spine that may be pressing on your spinal cord to give your spinal cord more room. However, this procedure may not be appropriate for all patients because it can lead to segmental instability and development of kyphosis. Your doctor may also choose an anterior cervical approach (through the front of your neck), which allows your doctor to directly see and remove any bone spurs and disc materials that may be pressing on your spinal cord. During surgery, your doctor may also perform a spinal fusion to reduce the risk of complications after surgery.
Read more about : Lower back pain symptoms & causes
Source :
 Posted in
Posted in 



0 comments:
Post a Comment